
The guide you read last year is out of date. The FDA resolved the semaglutide shortage in February 2025 and sent 55+ warning letters to compounding sellers by September. Truepill received a DEA Order to Show Cause in December 2022 over controlled-substance prescribing; the case was settled in November 2023 with heightened compliance measures, and the company was subsequently acquired in late 2024. Hims and Hers received a cease-and-desist from Novo Nordisk. Operators who built their entire program around a single compounding pharmacy or a single fulfillment partner got a very expensive education in what infrastructure resilience actually means.
The demand is still there. The GLP-1 market is projected to hit $40+ billion in North America by 2035, and patients are not going away. But the stack you need to capture that demand without regulatory and operational land mines is different from what worked in 2023. This guide reflects what we've learned from operating in this environment.
We've helped dozens of GLP-1 telehealth programs launch and scale. This is the layer-by-layer breakdown of what the stack actually looks like in 2026, including the specific failure points we've watched teams hit, the numbers that matter, and what we'd do differently if we were starting from scratch today.
The Seven Layers of a GLP-1 Stack
Every GLP-1 program, regardless of size, needs to solve seven problems. Some teams use one platform to cover multiple layers, others assemble best-in-class tools. Either way, you need real coverage across all seven. A gap at any layer costs you either revenue, patients, or your ability to operate legally:
- 01.Marketing site: how patients find you and decide you're legitimate
- 02.Checkout and intake: how patients pay, enroll, and submit health information
- 03.Provider network: who evaluates patients and writes the prescriptions
- 04.Pharmacy and eRx: how prescriptions get filled and shipped compliantly
- 05.Patient portal: how patients track their treatment, see their titration schedule, and manage refills
- 06.CRM and data routing: how patient data flows between systems without falling through the cracks
- 07.Analytics: how you measure conversion, churn, and cohort retention before problems become crises
Let's walk through each one.
1. Marketing Site
What Does a GLP-1 Marketing Site Do?
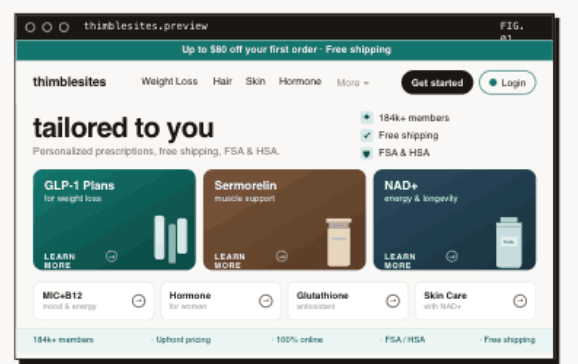
Your marketing site is where organic search converts, where paid traffic lands, and where patients decide whether your program feels legitimate. In GLP-1, trust signals matter more than in almost any other vertical. A patient who is considering injecting a medication weekly based on a 10-minute async consultation is doing a lot of credibility assessment before they click buy. Your site either passes that assessment or they bounce to a competitor.
What Makes a GLP-1 Marketing Site Convert in 2026?
Three things: speed, LegitScript certification, and structured trust signals. On speed: a site that scores below 80 on Lighthouse mobile is losing a measurable share of conversions. We've seen operators move from low to high Lighthouse scores and track meaningful lifts in checkout starts from the same paid traffic. That lift is free money. Your cost per acquisition drops without touching the ad budget.
On LegitScript: Google requires LegitScript certification to run ads for telehealth programs and prescription drug services. If you want Google Ads or Meta Ads for GLP-1, LegitScript is not optional. It's not a nice-to-have credential. Without it, your ads get disapproved or your account gets suspended. Build your site to pass the LegitScript certification requirements from day one rather than retrofitting it later.
Common GLP-1 Marketing Site Mistakes
Using a bloated page builder that loads 2MB of JavaScript before the patient sees anything. Skipping structured data markup that powers your appearance in "GLP-1 near me" and "semaglutide online" search results. Treating the marketing site as a brochure instead of a conversion funnel with measurable steps. And building without LegitScript in mind, which means you launch, apply for certification, get denied for something structural, and spend three weeks rebuilding what could have been right from the start.
This is one layer where custom work pays for itself quickly. A conversion-focused site built for performance (90+ Lighthouse scores, fast LCP, clean markup for structured data) will outperform a template every time, not in theory but in tracked checkout conversion. Thimble Sites is built specifically for this: healthcare operators who need performance, LegitScript compatibility, and conversion architecture, not a generic template with a custom header.
2. Checkout and Intake
What Does GLP-1 Checkout and Intake Do?
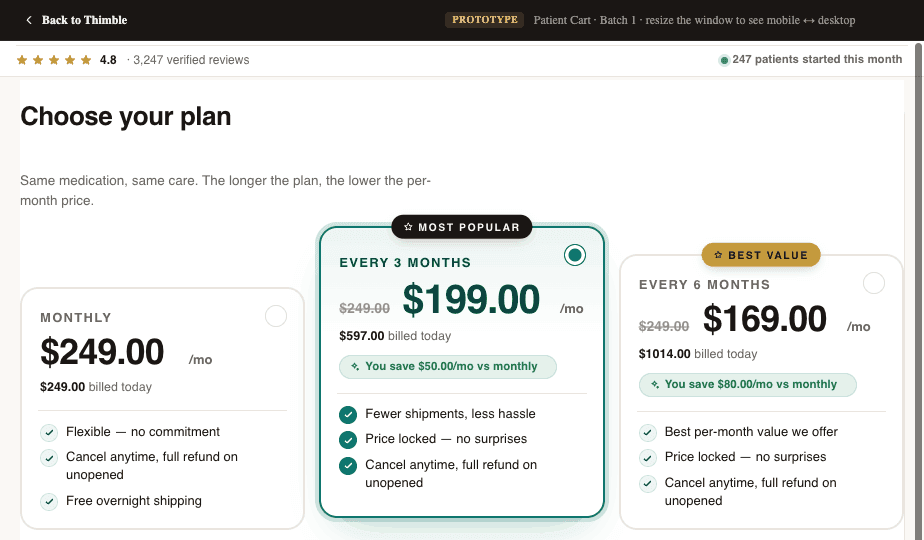
Checkout and intake is where the patient goes from interested to enrolled. They select a program, enter payment, and complete their medical questionnaire. It is the single highest-leverage piece of your stack. A 5% improvement in checkout completion is worth more than almost any other optimization you can run. It compounds across every patient you ever acquire.
What Makes GLP-1 Checkout and Intake Work?
Offer flexibility and wallet support. GLP-1 programs are complex commercial products. You need subscriptions with different billing cycles, tiered dosing plans that change price as patients titrate up, membership models, add-ons for lab work or supplies, and upsells for adjacent services. Your checkout needs to handle this cleanly without duct tape.
FSA and HSA payment support has become a meaningful revenue factor. A significant share of GLP-1 patients pay through FSA or HSA accounts, particularly employer-covered patients who recently got GLP-1 added to their benefits. If your checkout doesn't accept FSA/HSA cards (which requires specific merchant category codes and sometimes dual processing), you're turning away patients who have the budget and the motivation. Apple Pay and Google Pay express checkout consistently show meaningful conversion lifts on mobile. These are not nice-to-haves in 2026.
For intake forms, Formsort is purpose-built for healthcare with conditional logic and HIPAA compliance. Typeform works for simpler flows. Cognito Forms handles complex conditional logic at a lower price point and is underrated for teams with tight budgets.
Thimble Cart handles custom checkout flows with subscriptions, one-time purchases, memberships, tiered plans, add-ons, and upsells. It integrates with intake forms, provider networks, and payment processors (Stripe, Braintree, Authorize.Net), and it supports FSA/HSA processing. It's designed to work with any provider network and any pharmacy, so you're not locked into a single fulfillment path.
3. Provider Network
What Does a GLP-1 Provider Network Do?
The provider network is who actually evaluates patients and writes prescriptions. Unless you're a medical group with your own clinicians, you're contracting with a provider network that supplies licensed prescribers in the states where your patients live. This layer is purely buy, not build. Building your own provider network is a regulatory and operational undertaking that almost no early-stage GLP-1 operator should attempt.
How to Choose a GLP-1 Provider Network in 2026
State coverage, turnaround time, clinical quality, and integration capabilities. The major players each have different strengths. OpenLoop and Wheel offer broad state coverage and are well-suited for high-volume programs. Wizlo and CareValidate are strong for flexible provider matching and specific credentialing workflows. MD Integrations works well for teams that want more control over the clinical relationship. SteadyMD is the choice for dedicated provider models where the same clinician sees your patients consistently.
On DEA telehealth rules: GLP-1 medications (semaglutide, tirzepatide) are not controlled substances, so the Ryan Haight Act's in-person examination requirement does not apply. However, many GLP-1 programs also offer adjacent services that do involve controlled substances (ADHD, anxiety, sleep). If you offer those, the DEA telehealth flexibilities extended through December 31, 2026, apply. Track this for your full service offering, not just GLP-1 specifically.
Common Provider Network Mistakes
Choosing a network based on per-consult cost without evaluating turnaround time. A network that charges $5 less per consult but takes 48 hours instead of 8 will cost you far more in patient drop-off and support tickets than you'll ever save. Patients who pay $300 and then wait three days to hear anything dispute the charge. We've seen this pattern kill conversion rates for programs that were otherwise well-built.
The other mistake: not confirming state coverage before running paid acquisition. If you're buying traffic in Florida and your network isn't credentialed in Florida, every patient you acquire there is a patient you can't serve. Confirm coverage state-by-state before you turn on ads in any state.
4. Pharmacy and eRx
How Does GLP-1 Pharmacy Fulfillment Work in 2026?
This layer is where the 2025 crackdown hit hardest, and where the stacks that survived are different from the ones that didn't. The FDA resolved the semaglutide shortage in February 2025. By April 22, 2025, 503A compounding pharmacies were required to stop routine compounding of semaglutide. 503B outsourcing facilities had until May 22, 2025. Programs built around compounded semaglutide as their core product needed to rebuild this layer fast.
At the same time, Truepill's DEA compliance issues (Order to Show Cause in December 2022, settled November 2023 with heightened oversight requirements, followed by acquisition in late 2024) meant programs relying on Truepill for controlled-substance fulfillment had to find alternatives under pressure. The lesson was not that Truepill was uniquely bad. The lesson was that a single pharmacy dependency is a single point of failure, and this market has demonstrated it will exercise those failure points.
What Makes GLP-1 Pharmacy Fulfillment Reliable?
For eRx routing, DoseSpot and DrFirst are the two dominant platforms. Most provider networks already integrate with one or both. For fulfillment, Alto Pharmacy offers a consumer-facing experience with real-time delivery tracking. Specialty and mail-order pharmacies that carry brand-name Wegovy and Zepbound through proper channels are now the compliant path for GLP-1 programs. For programs that still operate in the compounded space (which requires documented medical necessity on a patient-by-patient basis, not a general business model), relationships with PCCA-member 503A pharmacies with strong compliance programs are essential.
Pharmacy Diversification Is Not Optional
Build relationships with at least two pharmacy partners from day one. Not because you're expecting to need both simultaneously, but because the cost of being wrong about your single pharmacy partner's stability is measured in weeks of patient disruption and potential chargebacks. The programs that came through the 2025 crackdown with the least damage were the ones that had already built a fallback. Alto for direct-to-patient fulfillment, a regional specialty pharmacy for overflow, and documented processes for switching between them.
5. Patient Portal
What Does a GLP-1 Patient Portal Do?
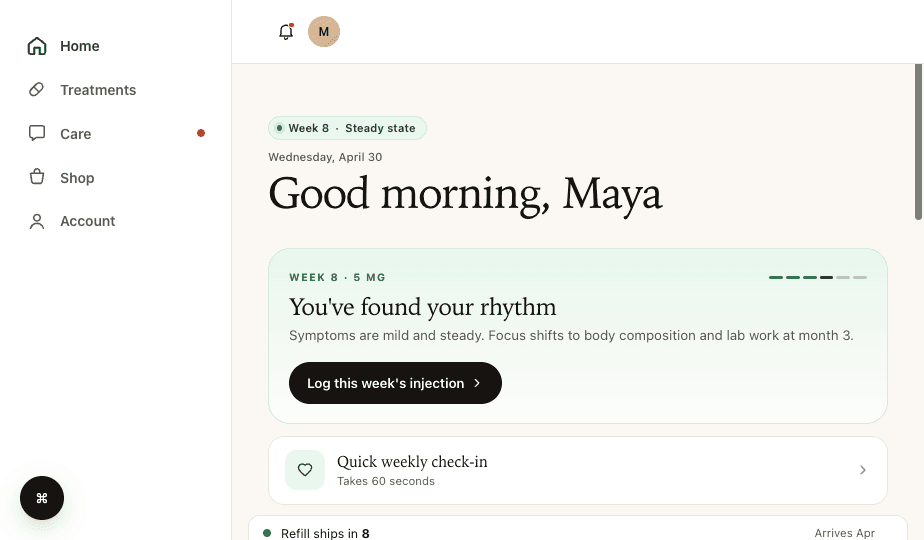
The patient portal is the ongoing experience after enrollment. It's where patients check order status, message support, request refills, and manage their account. For subscription programs, the portal is where retention happens. It's also where the gap between what a patient expects and what they actually get is most visible.
What GLP-1 Portals Need That Generic Portals Don't Have
Dosage and titration tracking. GLP-1 patients are on a titration schedule that typically starts low (0.25mg weekly for semaglutide) and escalates over months. They need to see exactly where they are in that schedule, when they move up, and what dosage they're currently on. This is not the same as a standard order status display. It's clinical context that patients need to understand their own treatment. Generic EHR patient portals do not display this information in a patient-friendly way.
Beyond titration tracking, the portal needs clear status at every stage: intake submitted, provider review, prescription sent, pharmacy fulfillment, shipped, delivered. The number-one driver of support tickets in GLP-1 programs is "where is my medication?" A portal that answers that question before the patient has to ask eliminates a large share of support volume. We've seen teams cut support ticket volume by 40% by adding accurate status tracking to their portal.
For the EHR layer, Healthie is excellent for telehealth-native workflows and has a modern API. Elation Health and athenahealth are stronger if your clinical team prefers a traditional interface. Canvas Medical is the developer-friendly, API-first option for teams that want maximum control over the patient data model.
Thimble Portal provides the patient-facing layer: accounts, status tracking, titration schedule display, messaging, refills, and follow-up assessments. It's designed to sit on top of whatever EHR or CRM you're running. It is not a replacement for your clinical system. It's a better front end for your patients.
Common Patient Portal Mistakes
Treating the portal as an afterthought and sending patients to a generic EHR portal that was not designed for DTC. Your checkout was branded and high-quality. If the portal looks like a 2012 medical records system, the contrast alone generates distrust and churn. The gap between a polished checkout experience and a clunky portal is where cancellations live.
6. CRM and Data Routing
What Does CRM and Data Routing Do in Telehealth?
The CRM layer is the connective tissue of your stack. It's where patient data lives, where automations trigger, and where your operations team manages the day-to-day. It is also the layer where most stacks fall apart, and where the failure is least visible until it becomes a patient crisis.
What Makes Telehealth Data Routing Work?
Clean, monitored data flow between every system. When a patient completes checkout, their information needs to route to your CRM, trigger a provider assignment, notify the clinical team, and route the prescription to the pharmacy. When the pharmacy ships, the tracking status needs to flow back to the patient portal. Every gap in that chain creates either a manual task for your team or a confusing silence for your patient. Patient silence turns into disputes.
For refill management specifically, automation is not optional at scale. A 200-patient program can handle refill outreach manually. At 500 patients, you cannot. You need automated sequences for refill reminders, payment failure recovery, and renewal consultation scheduling. Payment failure recovery automated within the first 48 hours of a failed charge recovers a meaningful share of otherwise lost revenue.
For the CRM itself, Tellescope is purpose-built for telehealth and handles patient communication, task management, and care coordination well. HubSpot and Salesforce are the enterprise options. GoHighLevel is popular with smaller operators who want an all-in-one marketing and CRM platform, though it requires customization for healthcare workflows.
For connecting everything together, automation platforms are essential, but the HIPAA constraint sharply narrows the field for any workflow that touches PHI. Zapier and Make have broad integration libraries but do not offer HIPAA-compliant plans and cannot sign BAAs, so they should be limited to non-PHI workflows like Slack notifications, marketing automation, or operational alerts. For PHI-touching automations, the realistic options are Keragon (healthcare-specific, BAA-eligible), self-hosted n8n inside your own controlled environment, or direct API integrations.
Common Data Routing Mistakes
Building automations that fail silently. A Zapier workflow that errors at 2 AM means a patient doesn't get routed to a provider, which means a 24-hour delay they weren't told about, which means a support ticket or a dispute. Monitor your automations with alerts, retry logic, and fallback handling. Treat them like production infrastructure, because that's what they are.
7. Analytics and Lab Integration
What Do Analytics and Labs Cover in a GLP-1 Program?
Analytics in a GLP-1 program covers business metrics (conversion, churn, LTV, cohort retention) and clinical data (lab results, dosing outcomes, patient-reported progress). For programs that require lab work, which is increasingly standard as programs mature and as payers push for outcomes documentation, you also need lab integrations.
What Metrics Matter Most for GLP-1 Programs in 2026?
On the lab side, Health Gorilla is the leading aggregator for electronic lab ordering and results retrieval, connecting to both Labcorp and Quest Diagnostics. If your program requires baseline metabolic panels or A1C testing before prescribing, you need a clean integration here. Some provider networks handle lab ordering natively; others expect you to manage it separately.
On business analytics, the four metrics that decide whether your program is healthy: checkout conversion rate from checkout start to payment complete (for warm traffic, typical telehealth programs see meaningful room between good and poor performers), time from payment to medication delivered (mail-order brand-name GLP-1 can be under a week for well-run programs), 90-day refill rate by cohort (a low rate is a retention problem, not a market problem), and support ticket volume per active patient per month (elevated rates typically mean your portal or status tracking has gaps).
Churn prediction is increasingly important for GLP-1 programs at scale. The patients most likely to cancel before month three have a specific behavioral signature: they don't log into the portal, they don't complete their follow-up assessment, and they're slower to request refills. If you can identify these patients at week four instead of week ten, you have time to intervene with a check-in sequence that saves a meaningful share of them. This requires cohort-level analytics, not just aggregate metrics.
How the Layers Connect
Understanding each layer individually is the easy part. The hard part, and the part most teams underestimate, is how the layers connect. The core data flow looks like this: patient lands on your marketing site, clicks through to checkout, selects a plan, enters payment, completes medical intake. Intake routes to CRM, triggers provider assignment. Provider reviews intake and writes a prescription. Prescription routes via eRx to pharmacy. Pharmacy fills and ships. Shipping status flows back through CRM to patient portal. Patient sees their status in real time.
Every arrow in that chain is a potential failure point. And when something breaks, the patient doesn't see a technical error. They see silence. No update, no medication, no communication. That's when they dispute the charge and file a complaint.
This is exactly why we built Thimble Cart, Thimble Sites, and Thimble Portal as modular products that integrate with best-in-class tools at every layer. You shouldn't have to use our pharmacy or our providers. You should be able to use whatever works best for your program and have the data flow cleanly regardless of what you pick.
Build vs. Buy: A Layer-by-Layer Decision
Not every layer deserves the same approach. Here's how we think about the build-vs-buy decision for each one:
- Marketing site: Build custom. This is your brand and your primary conversion surface. A performance-optimized site built for LegitScript certification and 90+ Lighthouse scores will outperform any template, and the investment pays back in lower acquisition costs for the life of the program.
- Checkout and intake: Buy or partner, but demand customization. Your checkout needs to feel like your brand, handle your specific offer structure, support FSA/HSA, and integrate with your specific provider and pharmacy partners. Off-the-shelf generic checkout doesn't handle all of this.
- Provider network: Buy. Building your own provider network is a regulatory and operational burden that almost no program should take on before product-market fit. Use an established network.
- Pharmacy and eRx: Buy, and build at least one redundant relationship. No custom building here. The compliance and logistics complexity makes this a pure partnership decision. Have a primary and a fallback.
- Patient portal: Build custom or use a purpose-built tool. This is a retention surface and it needs to feel like your brand. Include GLP-1-specific features like titration schedule display. Generic EHR patient portals were not designed for DTC and they show.
- CRM and data routing: Buy the CRM, invest heavily in the routing. The CRM platform matters less than the quality of your automations and integrations. Pick a CRM your ops team can work in, then invest in building reliable, monitored data flows with refill automation from day one.
- Analytics and labs: Buy. Use Health Gorilla or direct lab integrations for clinical data. For business analytics, instrument your stack with events and build cohort dashboards. Add churn prediction as soon as you have 90 days of patient data.
The Modular Advantage in a Volatile Market
The GLP-1 market has demonstrated, specifically and repeatedly, that pharmacy partnerships change, provider networks update their APIs, and regulations shift faster than most operators expect. The programs that came through 2025 in the best shape were the ones that could adapt without rebuilding from scratch.
A modular stack gives you that flexibility. If your pharmacy partner has supply issues, you switch to your fallback without touching your checkout or patient portal. If a new provider network offers better turnaround times, you onboard them without rewriting your intake flow. If the regulatory environment changes what you can offer, you update your checkout offers without rebuilding your entire site.
// PULLQUOTEThe goal isn't to find one platform that does everything. It's to pick the best tool for each layer and make sure they talk to each other reliably, with a documented fallback at every layer that matters.
That's the philosophy behind what we build at Thimble Hub. Thimble Cart handles checkout and intake with the flexibility to support any offer structure and any downstream partner. Thimble Sites delivers marketing sites that convert and pass LegitScript certification requirements. Thimble Portal gives patients a polished experience with GLP-1-specific features like titration tracking, without requiring you to rip out your existing clinical systems.
Each piece works independently. Together, they give you a stack that's built for the actual reality of running a GLP-1 program: not the pitch deck version, but the version where pharmacy supply chains get disrupted, FDA enforcement actions arrive with 90-day compliance deadlines, and patients expect Amazon-level tracking on a $350 monthly subscription.
Where to Start
If you're launching a GLP-1 program today, start with the three layers that touch the patient directly: your marketing site, your checkout and intake flow, and your patient portal. Get those right first. They determine your conversion rate, your first impression quality, and your retention. Those three metrics decide whether your program scales or stalls.
Then build out your provider network relationship, pharmacy integration (with a fallback), and CRM routing. These are the operational layers that determine how reliably you fulfill what you sold. They're less visible to the patient but they're what keeps the machine running through supply disruptions and regulatory changes.
The stack you launch with does not have to be the stack you run forever. But the architecture decisions you make now (modular vs. monolithic, custom vs. template, single pharmacy vs. diversified) are much harder to change under pressure. Get the architecture right, and the individual tools can evolve as your program grows and as the market continues to shift.
Frequently Asked Questions
- What technology do you need to launch a GLP-1 telehealth program in 2026?
- A complete GLP-1 stack needs seven layers: a marketing site (with LegitScript-compatible architecture), checkout and intake (with FSA/HSA support and unified flow), a provider network, pharmacy and eRx (with at least one fallback pharmacy relationship), a patient portal (with dosage and titration tracking), CRM and data routing (with automated refill management), and analytics (with cohort retention and churn prediction). The biggest change from 2024 is the pharmacy layer: programs that relied solely on compounded semaglutide needed to rebuild their fulfillment relationships after the FDA resolved the shortage and enforcement actions began.
- What provider networks work best for GLP-1 prescriptions?
- OpenLoop and Wheel offer broad state coverage for high-volume programs. SteadyMD is strong for dedicated provider models where continuity of care matters. Wizlo and CareValidate handle flexible provider matching and specific credentialing workflows. MD Integrations works well for teams wanting more control over the clinical relationship. Choose based on state coverage, turnaround time (best-in-class is same-day review), and integration depth, not per-consult cost alone. A network that is $5 cheaper per consult but takes 48 hours longer will cost more in patient drop-off than you'll ever recover in consult fee savings.
- How much does it cost to build a GLP-1 telehealth stack?
- All-in-one platforms typically charge monthly SaaS fees plus per-patient costs, often $5,000-15,000/month for programs above 200 active patients. Custom builds run six figures in upfront development plus ongoing maintenance. See /pricing for current Thimble Hub pricing. The biggest hidden cost across all approaches is data routing and integration engineering: budget for it explicitly before launch. Programs that treat it as a postscript routinely spend 2-3x more than planned getting their systems to actually talk to each other.
- Can pharmacies still compound semaglutide for GLP-1 telehealth programs?
- Only in documented cases of individual medical necessity, not as a general business model. The FDA resolved the semaglutide shortage in February 2025, which eliminated the legal basis for routine compounding by 503A and 503B pharmacies. 503A pharmacies were required to stop by April 22, 2025. 503B outsourcing facilities by May 22, 2025. The FDA sent 55+ warning letters to online sellers who continued marketing compounded semaglutide after the shortage resolutions. Programs building their business around compounded GLP-1s need to transition to brand-name medications through licensed pharmacy channels or diversify into other treatment categories.
- How long does it take to launch a GLP-1 program?
- Timeline depends heavily on how many layers you're building from scratch versus plugging into existing infrastructure. With a fully custom build, expect 4-6 months minimum to get all seven layers functioning and integrated. With modular infrastructure like Thimble Hub layered on top of existing provider network and pharmacy relationships, most programs can get to first patient in 4-8 weeks. The limiting factor is usually not the technology: it's LegitScript certification (4-8 weeks from application to approval) and provider network credentialing (2-6 weeks depending on the network and your states). Start those processes in parallel with your build, not after it.
Building a telehealth brand?
Thimble Hub gives you the checkout, intake, patient portal, and EHR-routing infrastructure so you can launch in weeks, not quarters. Modular, HIPAA-ready, no lock-in.