
If you run a clinic with 1 to 15 providers, the telehealth market probably feels like it was built for someone else. The enterprise platforms want six-figure annual contracts. The DIY approach means stitching together a dozen tools that don't talk to each other. And the 'simple' solutions turn out to be simple because they cut corners on compliance, patient experience, or both.
Meanwhile, your patients are asking for virtual visits. Your competitors are offering them. And every month you wait is another month of losing patients to clinics that figured it out first.
This guide is for you. Not for hospital systems with dedicated IT departments. Not for venture-backed telehealth startups with unlimited engineering budgets. For the clinic owner or practice manager who needs telehealth that works, at a price that makes sense, without a year-long implementation.
Why Enterprise Telehealth Doesn't Work for Small Clinics
The fundamental problem with enterprise telehealth platforms is that they're designed for scale that small clinics will never reach. They charge per-seat fees that assume hundreds of providers. They require implementation teams that bill by the hour. Their 'standard' onboarding takes 3 to 6 months because they're built for organizations with procurement departments and change management committees.
For a 5-provider practice, that model is absurd. You don't need a dedicated customer success manager to hold weekly status calls. You need a system that works on day one.
- Per-seat licensing eats your margin: At $200 to $500 per provider per month, a 10-provider clinic is spending $24,000 to $60,000 annually before seeing a single virtual patient.
- Implementation timelines kill momentum: When your competitor launches in two weeks and you're still in 'discovery phase,' you've already lost patients.
- Feature bloat creates training overhead: Enterprise platforms pack in features designed for hospital systems. Your front desk staff doesn't need 47 modules; they need scheduling, intake, and billing that work together.
- Contract lock-in removes your leverage: Multi-year contracts with early termination fees mean you're stuck even when the platform stops meeting your needs.
What Small Clinics Actually Need From Telehealth
Strip away the enterprise marketing and the feature comparison charts. What a small clinic actually needs is straightforward. You need patients to be able to find you, complete intake, pay, get treated, and come back. Everything else is either supporting those five steps or it's overhead.
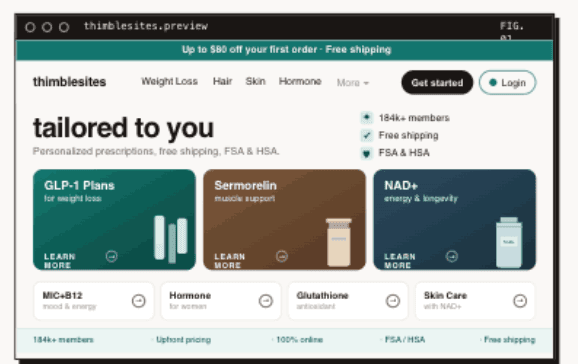
A Conversion-Optimized Front Door
Your website isn't a brochure. It's your front door. For telehealth, it's often your only door. If your site loads slowly, looks outdated, or makes patients work to figure out how to book, you're losing them before they ever see a provider. Moving from a low-performing site to one that scores 90+ on Google's Lighthouse performance test can produce meaningful conversion improvements.
Small clinics need sites that load fast, communicate clearly, and funnel visitors toward booking or checkout without friction. That means mobile-first design, fast page loads, and a clear path from 'I'm interested' to 'I'm a patient.'
Intake That Doesn't Lose Patients
The intake-to-checkout handoff is where most small clinic telehealth setups break down. A patient fills out a form on Typeform. Someone manually enters it into the EHR. Someone else sends a payment link. By the time the patient gets their first appointment, they've interacted with three different systems and received four different emails from four different sender addresses. Each handoff is a chance for them to drop off.
What you need is intake that flows directly into checkout, which flows directly into your provider system. One experience. Zero manual data entry. The patient fills out their information once, pays once, and lands in your system ready to be seen.
Compliance Without a Compliance Department
HIPAA compliance is non-negotiable, but it shouldn't require a dedicated compliance officer. Small clinics need infrastructure where HIPAA is the default, not an add-on. That means encrypted data at rest and in transit, signed BAAs included with your platform agreement, and audit logging that happens automatically rather than requiring manual configuration.
If your current setup requires you to think about whether a particular workflow is HIPAA-compliant, the setup is wrong. Compliance should be invisible because it's built into every layer of the system.
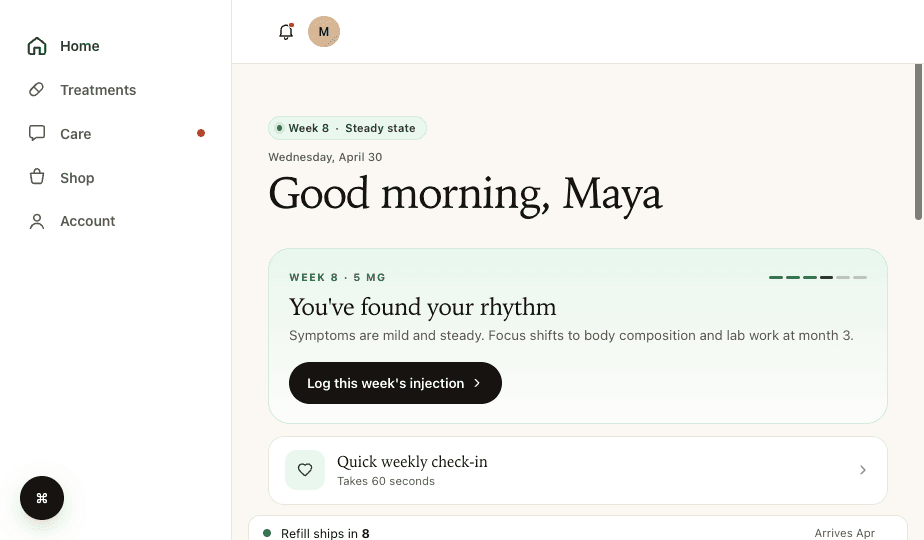
A Patient Portal That Drives Retention
The first visit is easy. Getting patients to come back for month two, three, and twelve is where small clinics struggle. In our internal data from Thimble Portal-powered programs, a patient portal that shows treatment progress, makes refills easy, and lets patients message their care team without calling your front desk is associated with dramatically better retention compared to email-and-phone-only follow-up.
For GLP-1 and weight management programs especially, patients who can see their dosage progression and track their results stay dramatically longer than patients who feel like they're just receiving a monthly shipment with no connection to their care team.
The Real Cost of Telehealth for a Small Practice
Let's talk actual numbers. Most 'how much does telehealth cost' articles are deliberately vague. Here's what a realistic budget looks like for a small clinic in 2026.
The DIY Patchwork Approach
- Video platform (Zoom for Healthcare, Doxy.me): $15 to $100/month per provider depending on plan tier
- Intake forms (Typeform, JotForm): $50 to $100/month
- Payment processing (Stripe + custom integration): $500 to $2,000 setup + ongoing fees
- Patient portal (basic EHR portal or none): $0 to $300/month
- HIPAA compliance (managed IT + BAAs): $700 to $2,500/month
- Website updates and maintenance: $200 to $500/month
- Staff time stitching it all together: 10 to 20 hours/week
Total: roughly $2,000 to $5,000 per month in direct costs, plus significant staff time. And none of it talks to each other, so you're paying for integration overhead forever.
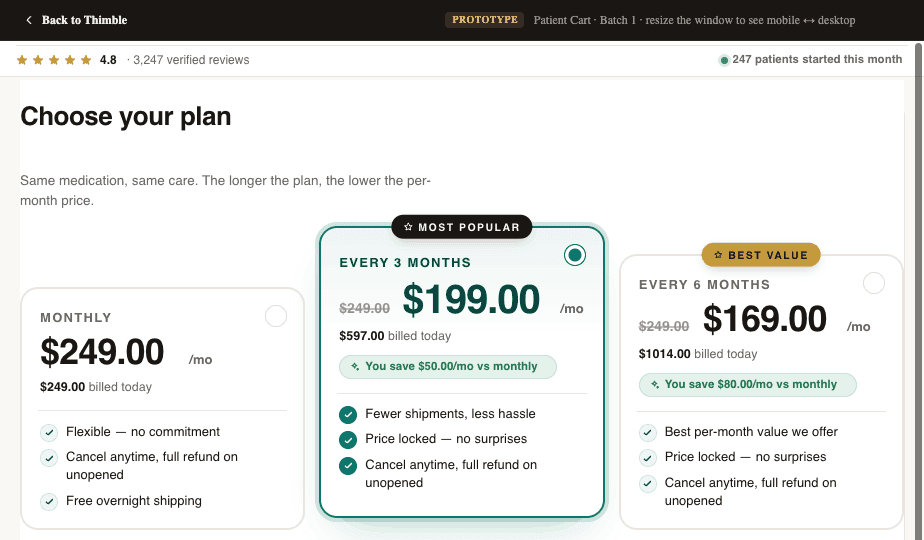
The Modular Infrastructure Approach
A modular approach means picking purpose-built components that integrate natively. Your checkout handles intake and payment in one flow. Your portal handles patient experience and retention. Your site handles conversion. Each piece does its job well, and the data flows between them automatically.
The upfront investment is higher than the DIY approach, but the ongoing costs are lower because you're not paying for manual workarounds. More importantly, you're not losing patients at every handoff point between disconnected tools.
How to Launch Telehealth in Under a Month
The biggest mental barrier for small clinics is the assumption that telehealth takes months to set up. It doesn't. Not if you choose the right infrastructure.
Week 1: Foundation
- Choose your provider network (or use your existing providers with a video platform)
- Set up your checkout and intake flow with your treatment programs configured
- Connect your payment processing (Stripe, with FSA/HSA support if you serve self-pay patients)
- Configure your patient communications (welcome emails, appointment reminders)
Week 2: Patient Experience
- Configure your patient portal with treatment tracking and messaging
- Set up automated refill flows and subscription management
- Build your marketing site or connect your checkout to your existing site
- Test the full patient journey end-to-end: intake, checkout, provider assignment, portal access
Week 3: Optimization
- Launch with a small patient cohort and monitor the full workflow
- Set up analytics to track conversion rates, retention, and operational bottlenecks
- Configure automation rules (follow-up emails, payment failure recovery, appointment reminders)
- Train your staff on the admin dashboard and patient management tools
By week four, you should be serving patients and iterating on the experience. Not writing requirements documents. Not sitting through vendor demos. Actually treating patients.
Choosing the Right Telehealth Verticals
Not every specialty translates equally well to telehealth. For small clinics, the best verticals share three characteristics: high patient demand for virtual access, subscription-friendly treatment models, and manageable regulatory complexity.
- Weight management and GLP-1 programs: Enormous patient demand, subscription billing model, clear treatment protocols. The fastest-growing telehealth vertical by revenue.
- Hormone therapy (TRT, HRT): Ongoing treatment with regular follow-ups. Patients prefer the convenience of virtual visits for what is essentially medication management.
- Mental health and behavioral health: Interstate compacts (PSYPACT covers 40+ jurisdictions as of 2026) make multi-state practice feasible. High demand consistently outstrips provider supply.
- Dermatology: Asynchronous consults (photo-based) work well for many conditions. Good entry point for clinics testing telehealth without live video infrastructure.
- Primary care follow-ups: Not a standalone telehealth play, but adding virtual follow-ups to an existing in-person practice dramatically improves retention and reduces no-shows.
The Multi-State Expansion Opportunity
One of the biggest advantages telehealth gives small clinics is the ability to serve patients beyond your geographic area. Interstate licensure compacts have expanded significantly. As of early 2026, the Interstate Medical Licensure Compact covers 40+ states, PSYPACT for psychologists covers 40+ jurisdictions, and the Nursing Licensure Compact covers 40+ states (verify current membership at each compact's official site, as these numbers change frequently). If your providers are licensed through these compacts, you can effectively multiply your addressable market overnight.
For a 5-provider clinic that previously served a single metro area, suddenly being able to treat patients across 40+ states is transformational. The infrastructure cost to support multi-state operations is negligible compared to opening physical locations. You need compliant intake, proper licensing verification, and a checkout system that handles state-specific requirements. That's it.
Avoiding the Common Traps
- Don't overbuild before you have patients. Start with the minimum viable telehealth setup: intake, checkout, provider, portal. Add complexity as your patient volume justifies it
- Don't sign multi-year contracts. The telehealth market is moving fast. What works today may not be the best option in 12 months. Annual contracts with monthly billing give you flexibility
- Don't ignore mobile. The majority of telehealth patients interact with your platform on their phone first. If your checkout or portal doesn't work flawlessly on mobile, you're losing patients
- Don't separate your brand. If patients see one brand on your website, a different experience at checkout, and a third brand in their portal, trust erodes. One brand across every touchpoint matters more than any individual feature
- Don't treat compliance as a Phase 2 concern. Building on non-compliant infrastructure and 'fixing it later' is how clinics end up with HIPAA violations and LegitScript certification failures. Start compliant from day one
The Bottom Line
Small-to-mid size clinics have a structural advantage in telehealth that most don't realize. You can move faster than hospital systems. You can personalize patient experiences in ways that enterprise platforms can't. You can launch in weeks, iterate based on real patient feedback, and build a telehealth practice that actually reflects your clinical approach rather than a vendor's template.
The clinics that win in telehealth aren't the ones with the biggest budgets. They're the ones that launch, learn, and iterate. And the right infrastructure makes that possible on the first try, not the third.
Frequently Asked Questions
- How much does it cost to add telehealth to a small clinic?
- Direct platform costs typically range from $1,500 to $5,000 per month depending on the components you need. The key is avoiding per-seat licensing models that scale costs with your provider count rather than your revenue. Factor in the cost of patient churn from disconnected systems when comparing options.
- How long does it take to launch telehealth?
- With the right modular infrastructure, most small clinics can go from zero to treating patients in 2 to 4 weeks. Enterprise platforms that quote 3 to 6 month timelines are reflecting their own complexity, not the inherent difficulty of telehealth.
- Do I need to replace my existing EHR to offer telehealth?
- No. A modular approach lets you keep your existing EHR, CRM, and other systems. The telehealth layer (intake, checkout, portal) integrates with your current stack rather than replacing it. This dramatically reduces both cost and disruption.
- Can a small clinic realistically serve patients in multiple states?
- Yes. Interstate licensure compacts now cover 40+ states for most provider types. The infrastructure cost of multi-state telehealth is minimal. The main requirements are proper licensing verification, compliant intake forms, and state-aware checkout configuration.
- What's the most important feature for patient retention in telehealth?
- A patient portal that gives patients visibility into their treatment, makes refills easy, and provides a direct messaging channel to their care team. In our internal data from Thimble Portal-powered programs, clinics with full-featured portals see substantially higher retention rates compared to clinics relying on email and phone follow-ups alone.
Building a telehealth brand?
Thimble Hub gives you the checkout, intake, patient portal, and EHR-routing infrastructure so you can launch in weeks, not quarters. Modular, HIPAA-ready, no lock-in.